

A primary care provider operates a multi-location network, including Atlanta and Georgia, where 15 clinical agents handle 13,000 weekly calls. These agents coordinate patient inquiries across Salesforce, Five9, and eClinicalWorks (eCW) and manually document telephone encounters during each call. Prescription refills generate the highest inbound volume, requiring agents to navigate disconnected software systems to verify medications. The previous interactive voice response (IVR) system routed all refill requests directly to human agents, regardless of whether the caller required clinical intervention. This structure forced the organization to pay for automated connection fees only to immediately hand the call to a high-cost clinical resource.
Manual verification requirements and rigid routing queues delayed urgent patient care
Clinical staff spent their shifts on routine, repetitive tasks while acute cases remained unprioritized in the queue. The previous routing logic handled all prescription requests identically, which introduced clinical risks for patients who required temporary bridge medications before their next scheduled appointment. Callers seeking services outside the contact center's scope, including prior authorizations, imaging results, and outbound faxes, remained on the line for 90 seconds while agents completed full identity verifications before initiating a transfer.
When transfers did occur, agents frequently duplicated documentation because Salesforce did not surface the existing telephone encounter. Misrouted calls forced patients to redial and navigate the same circular IVR menus, generating repeat contacts and operational bottlenecks. Supervisors lacked automated methods to identify abandoned calls or failure patterns, leaving them dependent on manual, individual call reviews to detect operational errors. Their contact center leader described the core issue:
"We're paying a ton of money to have an agent answer a phone call, get charged for a short amount of interaction time, and then still engage a human and double pay."
- Contact Center Leader
Level AI’s virtual agent integrates with eClinicalWorks and Salesforce to verify patients and prioritize urgent clinical refills
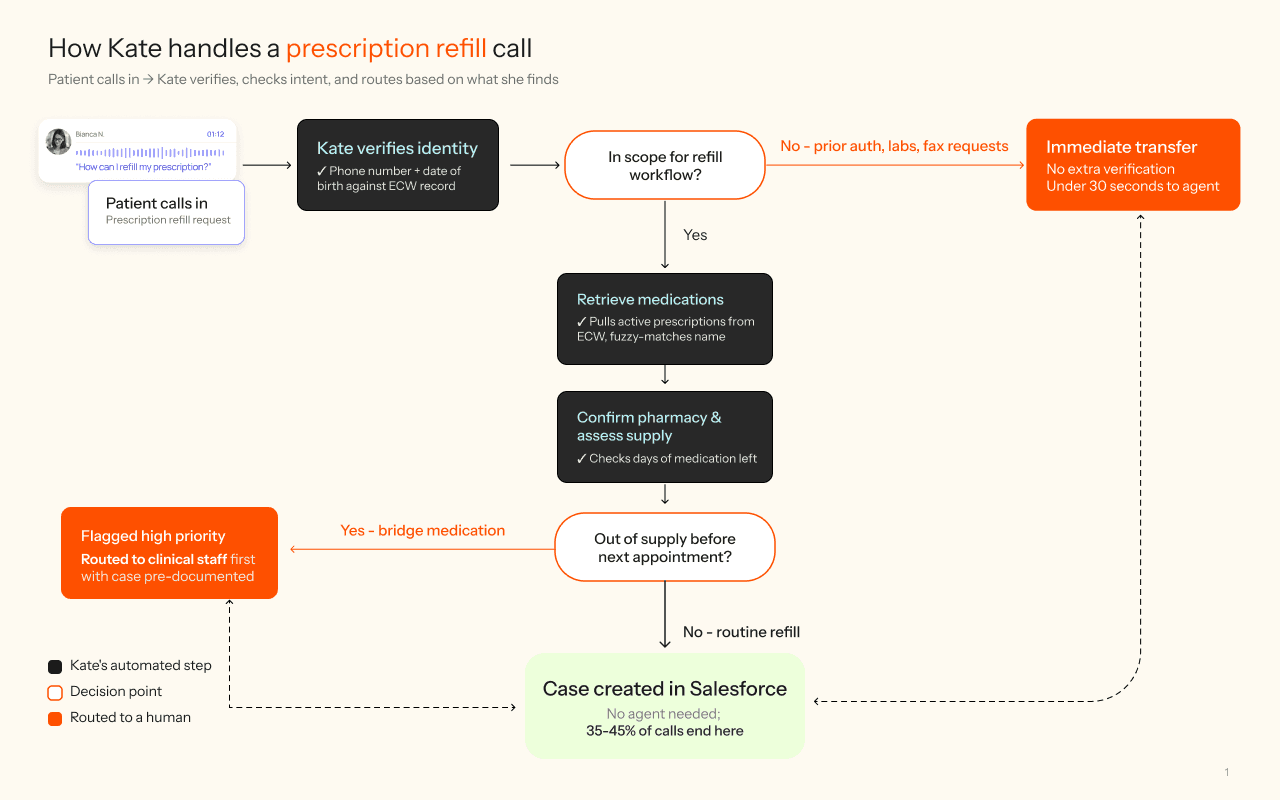
The primary care provider conducted a Proof of Concept (POC) with Level AI's Virtual Agent, integrated with Salesforce and eClinicalWorks (ECW). Now, when a patient calls, the Virtual Agent verifies identity using the phone number and date of birth before retrieving active medications and pharmacy details from ECW. The system then updated Salesforce with structured data, including the medication supply status and the telephone encounter.
Two workflow adjustments have been central to the ongoing POC. The team observed that the Virtual Agent initially ran full verification on calls it couldn't handle. Level AI’s team refined the pilot workflow to identify intent up front: for calls that fall outside the POC scope, the system is now designed to transfer within 30 seconds. Initial tests show that the average interaction time for out-of-scope calls has dropped from 90 seconds to under 30 seconds. The partnership is also evaluating fuzzy matching logic after a pilot case where a patient said "lipid drill" (lisinopril), and the system sought to improve matching accuracy.
Virtual Agent is currently processing a subset of the prescription refill call volume, managing 165 interactions on its first full day of pilot deployment. In cases requiring human escalation, the pilot aims to provide agents with a Salesforce record containing verified identity and medication lists to evaluate the reduction of duplicate documentation. A contact center lead commented on the pilot's early performance:
"It is faster because most of that is there... now they are paying more attention to it. And so then just adding from that case that's already created."
- Clinical Operations Lead
Routine request deflection frees clinical personnel for complex care and exposes operational bottlenecks
Early results from the pilot demonstrated that the Virtual Agent handled 45% of prescription refill calls without agent intervention. This deflection rate is a key metric being tracked as the pilot reached full traffic volume in early May. Clinical staff, freed from routine refill calls, now focus on cases that require clinical judgment.
Out-of-scope calls transfer in under 30 seconds, saving 983 hours in total conversation time. Patients calling about prior authorizations or imaging results, or faxing requests, no longer undergo unnecessary verification. The workflow identifies intent upfront and routes immediately.
High-priority cases get flagged automatically. The Virtual Agent identifies patients who will run out of medication before their next appointment and marks their telephone encounters as high priority, so clinical staff see urgent requests before routine ones.
The team gained visibility into Virtual Agent performance through custom dashboards. The contact center leader used custom dashboards to filter out pharmacy calls, surfacing the true deflection rate for in-scope workflows. The team also used conversation intent data to track which workflows succeeded and which needed refinement.
"I think you've proven in my eyes that you're able to deliver on what you say you can deliver on. Now, we just need to fine-tune and meet the metrics — that's the goal."
- Contact Center Leader
