

Key takeaways
The staffing misalignment: Staff in healthcare contact centers spend 60-70% of their time on routine tasks like appointment confirmations, prescription refill requests, and basic patient information updates that require zero clinical judgment. (Sequence Health, December 2025)
The real cost: At $21/hr (Salary.com, April 2026) and a 3 min 28 sec average talk time per call (HubSpot), routine calls cost approximately $340,000-$396,000 per year in agent salary alone at a 9,000 calls/week contact center.
The documentation burden: After-call work adds 60-90 seconds of wrap-up to every call. At 9,000 calls per week, that is an additional $164,000-$205,000 per year in agent salary spent purely on EMR entries, intake logging, and call tagging.
The right fix starts with your call data: Reviewing 100% of existing recordings reveals your actual call drivers, letting you map which workflows staff should own vs. which can be automated.
Done right, 80% of repetitive calls can be resolved without human involvement, covering scheduling, prescription refills, test result inquiries, and intake triage, with staff stepping in only when a patient genuinely needs them.
Introduction
If you run a healthcare contact center, you already know what happens at 8am on a Monday. The queue fills fast: appointment reschedules, prescription refill requests, test result questions, insurance queries, and yes, the occasional call about chest pain. Every one of them lands in the same place. Every one of them waits in the same line.
That architecture has a cost most organizations are not measuring.
Routing all inbound volume into a single queue means agents are spending the majority of their day on calls that require no clinical judgment whatsoever. Research shows that staff in healthcare contact centers spend 60-70% of their time on repetitive tasks like appointment confirmations, prescription refill requests, and basic patient information updates. (Sequence Health, December 2025) These are calls that do not need a trained agent. They need a workflow.
The cost of this misalignment compounds daily. When the majority of agents are fielding work that does not require human judgment, the math stops making sense quickly. Hold times stretch to 8-12 minutes, staff burn out faster. And patients with genuinely urgent concerns wait in the same queue as someone trying to move a Tuesday appointment.
If a virtual agent could pick up and suggest a doctor in their local area and book the appointment, that would be a major win
— Healthcare provider, multi-site primary care network
The real cost of not automating
Most contact center leaders frame the automation conversation around the cost of new technology. The more important number is what you are already spending on work that does not require a human. Using agent salary alone, the figure is significant.
FTE cost of misrouted calls
Medical Call Center Representatives in the US earn an average of $21/hour. (Salary.com, April 2026) The average talk time per call in healthcare is 3 minutes and 28 seconds. (HubSpot) That puts the agent salary cost at $1.21 per call in talk time alone.
At a contact center handling 9,000 calls per week, with staff spending 60-70% of their time on routine, non-clinical tasks (Sequence Health, December 2025), that means 5,400-6,300 calls per week are consuming agent time that a virtual agent could handle instead.
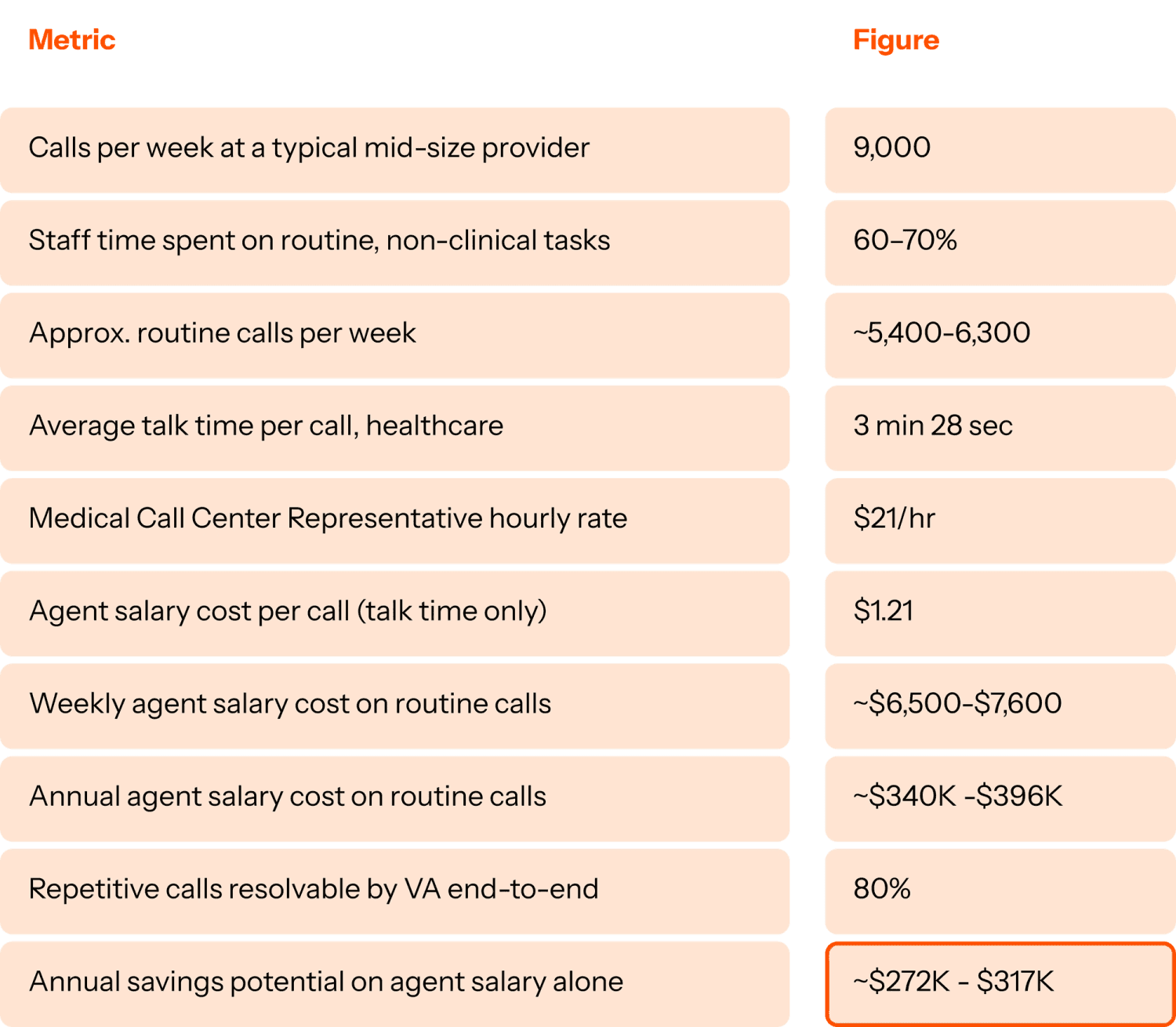
Even using the most conservative end of range, the math is stark: over $3M per year spent on calls that required zero clinical judgment. The cost table above only captures the call itself. It doesn’t count what happens after the patient hangs up. In healthcare contact centers, agents manually create telephone encounters in the EMR, log intake information, and route cases after every interaction, tasks that add 60–90 seconds of wrap-up time to every single call.
At 9,000 calls per week, that adds up fast:
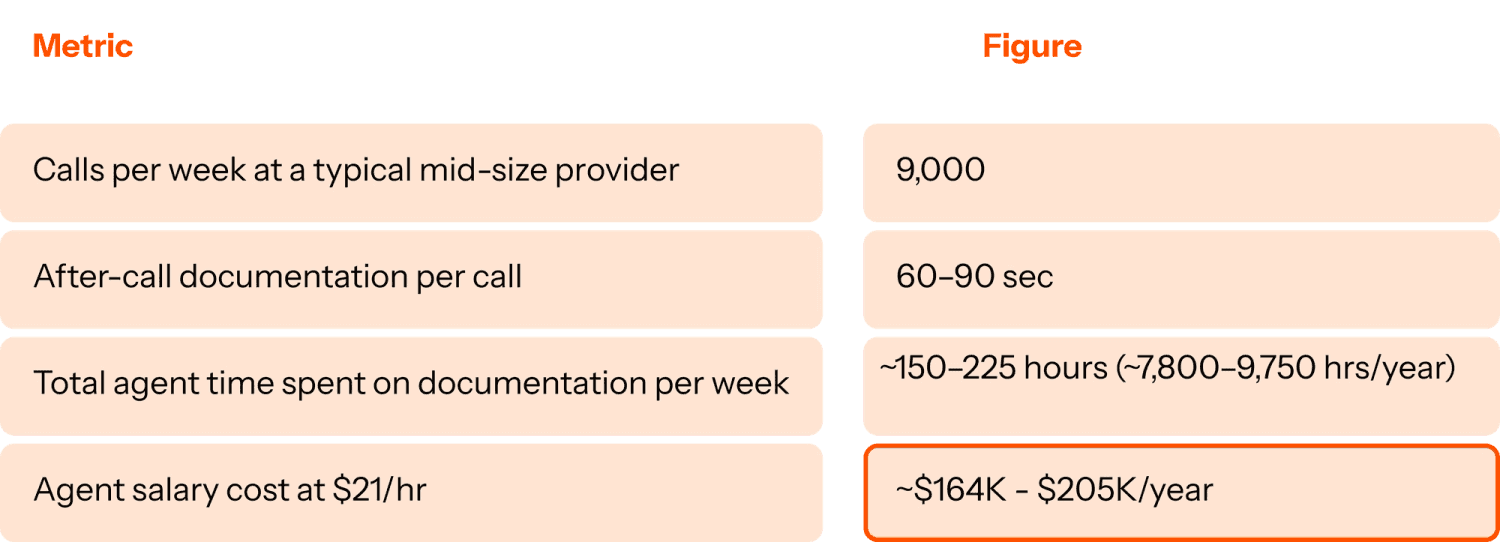
Up to $205,000 per year in agent salary spent writing up calls: creating EMR entries, logging intake notes, tagging call outcomes. Work that a purpose-built system handles automatically. This is the workflow architecture healthcare contact centers should solve for.
What the right automation looks like
The conversation about healthcare AI often gets stuck at the question of “which calls can we automate?” That’s the wrong starting point because it assumes you already know what your calls actually are.
The right approach starts with your data. A healthcare contact center software that mines 100% of your existing patient interaction recordings can identify your actual top call drivers - not what you think they are, but what they actually are - then map the exact workflow logic your best-performing agents use to resolve them. From there, you can identify which workflows are safe and profitable to automate versus which genuinely require clinical judgment.
The use cases that consistently emerge across provider organizations are:
Patient intake and triage: Initial verification, case creation in the contact center system, intelligent routing to the right clinical team, eliminating the non-clinical intermediary step entirely
Prescription refill requests: Identity verification, medication list query in EHR, controlled substance flagging for escalation, all before a human is involved
Test result inquiries: Intelligent deflection when labs are within normal turnaround SLA, escalation when they’re not
Appointment scheduling and rescheduling: End-to-end handling including after-hours, synced directly with the scheduling system
Medication management outreach: Verification and consent before nurse transfer, replacing manual non-clinical steps
This is, however, not a comprehensive or one-size-fits all exercise. The categories required to be automated depend on the workflow designs and type of calls the contact center handles everyday.
The Level AI approach: Mine before you build
Analyze 100% of existing call recordings to identify real call drivers
Map best-agent workflows for each automation candidate
Identify the precise boundary between automatable and clinical
Deploy pre-trained AI agents for mapped service flows, appointment confirmation, after-hours triage, prescription refill intake
Outcome: resolve 80% of repetitive calls end-to-end, no human required until one is genuinely needed
What to watch out for while deploying your AI Virtual agent
The healthcare automation market is growing fast and with that growth has come a proliferation of tools that automate one layer of the contact center without connecting to what happens before or after. Scheduling automation that doesn’t touch QA. Call deflection that doesn’t feed an intelligence loop. Bot performance that goes unmonitored while human agents are graded on different rubrics.
The risk isn’t choosing the wrong vendor. It’s deploying a solution that solves one problem in isolation and creates three others, a siloed AI system that can’t improve itself, can’t tell you why calls are escalating, and can’t get better from the intelligence already in your operation.
The question worth asking before any automation conversation is simpler than most vendors make it: what percentage of your calls actually require a human? Pull your call data. Segment it by whether each call type required clinical judgment. The number you find is usually the starting point for a very different kind of conversation about how to run your contact center.
This is part one of The Patient-First Contact Center: a four-part series for healthcare contact center leaders navigating AI. Next week: why most virtual agents fail in healthcare, and what purpose-built actually looks like.
Explore how healthcare contact centers are rethinking their automation strategy
This is part one of The Patient-First Contact Center, a four-part series for healthcare contact center leaders navigating AI.
Part 2: The risks of AI in healthcare (and what purpose-built AI actually looks like)
Part 3: Why siloed automation at healthcare contact centers fails at patient care
Part 4: Why AI deployment in healthcare takes 6-12 months and how to fix it
FAQ section
What percentage of healthcare contact center calls can be automated?
Research consistently shows that 60-70% of inbound patient calls including appointment scheduling, prescription refill requests, test result inquiries, and basic intake triage require zero clinical judgment and are candidates for automation. The remaining 30-40% involve clinical complexity, emotional nuance, or edge cases that require a trained human agent.
What is the average hold time in healthcare contact centers?
Average hold times in healthcare contact centers run between 8 and 12 minutes significantly higher than other industries. The primary driver is call volume misallocation: routine, automatable calls sit in the same queue as complex clinical inquiries, creating backlogs across the entire operation.
What types of patient calls can a virtual agent handle in healthcare?
AI agent for healthcare can handle appointment scheduling and rescheduling, prescription refill requests, test result status inquiries, patient intake and triage (initial verification and case creation), medication management outreach, and password resets for patient portal access. These use cases account for the majority of inbound call volume at most provider organizations.
How do you identify which healthcare contact center workflows to automate?
The most reliable approach is data-first: mine 100% of existing patient interaction recordings to identify actual call drivers, then map the workflow logic your best-performing agents use to resolve them. This surfaces the precise boundary between calls that are safe to automate and calls that require clinical judgment rather than guessing based on assumptions about call volume.
What is the cost of not automating a healthcare contact center?
The cost of inaction compounds across three areas: FTE spend on calls that don’t require clinical judgment, after-call work time spent on manual documentation (60-90 seconds per call at scale), and patient experience impact from hold times and repeated callbacks. For a mid-size provider handling 9,000 calls per week, 60% routine call volume means more than 5,000 calls per week consuming clinical staff time unnecessarily.
What is a virtual agent in healthcare?
A healthcare virtual agent is an AI-powered system designed to handle patient calls and messages end-to-end verifying patient identity, querying EHR systems, resolving routine requests, and escalating to human agents when clinical judgment is required. Unlike general-purpose chatbots, purpose-built healthcare virtual agents integrate directly with EHR and contact center platforms, follow clinical escalation logic, and are trained on real patient


